What Is Esophageal Cancer?
Esophageal cancer forms in tissues that line the esophagus, which is the hollow, muscular tube that moves food and liquid from the throat down into the stomach. Esophageal cancer starts at the inside lining of the esophagus and spreads through the outer layers as it grows.
Esophageal cancer is relatively uncommon in the United States, and it affects many more men than women. It is a challenging condition to treat, since patients usually aren't diagnosed until the cancer has advanced to the point where it causes symptoms. At Dana-Farber Brigham Cancer Center, about 60 percent of our esophageal cancer patients are diagnosed with metastatic cancer, meaning that it has spread to other organs and distant lymph nodes.
In the past two decades, our knowledge about esophageal cancer has improved dramatically. Physicians at the Center for Esophageal and Gastric Cancer at Dana-Farber Brigham Cancer Center have a clearer understanding of which patients are likely to benefit from a particular treatment approach or clinical trial, and can deliver a combination of surgery, chemotherapy, and radiation more precisely.

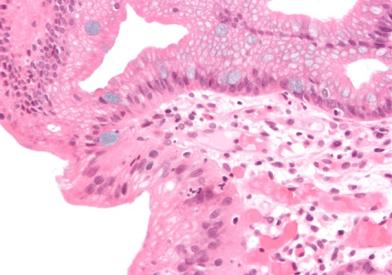
What Is Barrett's Esophagus?
Barrett's esophagus is a condition that can be pre-cancerous or, in a more advanced state, an early form of esophageal cancer. It is often the result of chronic inflammation due to acid reflux, and appears as abnormal cells lining the lower part of the esophagus. When it's found early, it presents an opportunity to prevent it from progressing into cancer.
Risk Factors
There's a misconception that the people at risk for developing esophageal cancer are primarily smokers and drinkers. While smoking and drinking do increase the likelihood of developing the squamous cell carcinoma variant of this cancer, in reality, the most common form of this cancer, adenocarcinoma, can afflict just about anyone. However, risk factors include:
- Males
- People with Barrett's esophagus
- People with gastroesophageal reflux disease (GERD)
- Obesity
- Smoking (including pipe and cigar)
Signs and Symptoms
The early stages of esophageal cancer usually don't produce any physical symptoms. By the time symptoms are noticeable, the disease has usually become advanced. The most common signs and symptoms are:
- Painful or difficult swallowing
- Weight loss
- Regurgitation of undigested food
When esophageal cancer is found very early, it is usually "accidental," meaning that patients are being medically examined for another reason when it's suspected and found, sometimes in a pre-cancerous form called Barrett's esophagus. When it's caught early, there is a much better chance of recovery.