What Is Hodgkin Lymphoma?
In Hodgkin lymphoma, a cancerous tumor develops in a lymph node, often in the neck or chest, although other lymph nodes can be affected. If Hodgkin lymphoma spreads, it usually spreads first to nearby lymph nodes, and then to the spleen, liver, or bone marrow. It is considered to be one of the most treatable cancers.
- Hodgkin lymphoma is a malignancy of a family of white blood cells known as lymphocytes.
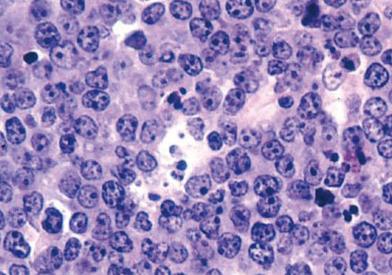
- It is marked by the presence of Reed-Sternberg cells, which are mature B cells that have become cancerous and unusually large, and carry more than one nucleus.
Adult Hodgkin lymphoma is a disease in which cancer cells form in the lymph system.
The lymph system is made up of the following:
- Lymph: Colorless, watery fluid that travels through the lymph system and carries white blood cells called lymphocytes. Lymphocytes protect the body against infections and the growth of tumors.
- Lymph vessels: A network of thin tubes that collect lymph from different parts of the body and return it to the bloodstream.
- Lymph nodes: Small, bean-shaped structures that filter lymph and store white blood cells that help fight infection and disease. Lymph nodes are located along the network of lymph vessels found throughout the body. Clusters of lymph nodes are found in the underarm, pelvis, neck, abdomen, and groin.
- Spleen: An organ that makes lymphocytes, filters the blood, stores blood cells, and destroys old blood cells. It is located on the left side of the abdomen near the stomach.
- Thymus: An organ in which lymphocytes grow and multiply. The thymus is in the chest behind the breastbone.
- Tonsils: Two small masses of lymph tissue at the back of the throat. The tonsils also make lymphocytes.
- Bone marrow: The soft, spongy tissue in the center of large bones. Bone marrow makes white blood cells, red blood cells, and platelets.
Treatments vary depending on the type of disease, its aggressiveness, and its location, along with your age and general health.
There are two main types of Hodgkin lymphoma:
- Classical: This is the most common form, and can be broken down into four subtypes: nodular sclerosing (the most common sub-type); mixed cellularity; lymphocyte depletion; and lymphocyte-rich.
- Nodular lymphocyte-predominant (NLPHL): A rare form of Hodgkin lymphoma that is a slow-growing disease.
Incidence
Hodgkin lymphoma is relatively rare, with about 9,000 new cases diagnosed each year in the United States. About 173,000 people currently living in the United States have had Hodgkin lymphoma at some point in their lives.
Growth and Spread
Because lymph tissue is found throughout the body, Hodgkin lymphoma can begin in almost any part of the body and spread to almost any tissue or organ. Hodgkin lymphoma tends to progress in a predictable fashion, moving from one group of lymph nodes to the next, and is often diagnosed before it reaches an advanced stage.
Risk Factors
Risk factors include:
- Being in young or late adulthood: Hodgkin lymphoma most often occurs in people ages 15 to 24 and in people over 60.
- Having a compromised immune system.
- Being male.
- Exposure to the Epstein-Barr virus.
- Having a first-degree relative (parent or sibling) with Hodgkin lymphoma, which may increase your risk slightly.
Hodgkin lymphoma may also occur in people who have acquired immunodeficiency syndrome (AIDS). These patients require special treatment and need to be monitored for drug interactions. Our infectious disease specialists work with us to plan care for people with both conditions.
Symptoms and Signs
The most common signs of Hodgkin lymphoma are swollen (painless) lymph nodes in the neck, underarm, or groin, as well as a fever, night sweats, and weight loss. Other symptoms can include itchy skin, fatigue, cough, or shortness of breath, but these symptoms are usually related to other medical factors.