The Colon and Rectal Cancer Center includes medical, surgical, and radiation oncologists, endoscopy specialists, gastroenterologists, radiologists, and pathologists who treat patients at all stages of the disease.
Your care team will collaborate to develop a comprehensive, personalized treatment plan that offers the most advanced therapies and an array of supportive resources.
Rectal cancer forms in the tissues of the rectum, which is the last several inches of the large intestine before the anus (the opening of the large intestine to the outside of the body). Most of the large intestine is called the colon.
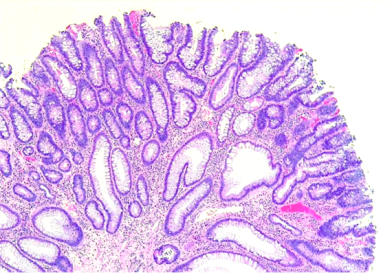
Rectal cancer usually develops over years, starting with precancerous growths called polyps. Some polyps grow to penetrate the wall of the rectum.
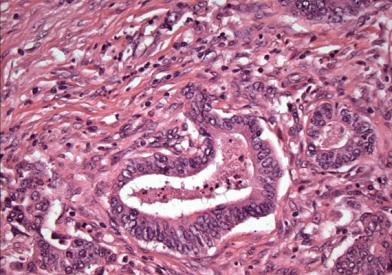
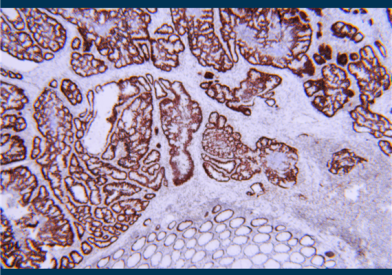
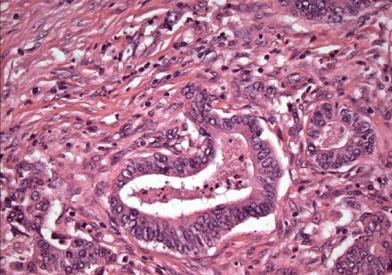
Different types of cancer can develop in the rectum. Most rectal cancers are adenocarcinomas, which are cancers from glandular tissue. Other cancer types that can occur in the rectum include carcinoid tumors, small cell carcinomas, and gastrointestinal stromal tumors (GIST).
The focus of this information is on rectal cancers that are adenocarcinomas.
Colon and rectal cancers are the fourth most common cancers diagnosed in the United States. Survival after diagnosis has been gradually increasing in the past decade for several reasons, including:
Screening programs can catch the disease in its pre-cancerous or early stages, which are more curable.
Increasingly, there are better therapies – both surgical techniques and chemotherapies, including targeted therapies.
Our team has been a leader in clinical trials for various treatments for rectal cancer, to improve outcomes for patients and survivors.
When detected early, rectal cancer is a very treatable form of cancer. The earlier that it is found, the more likely that it will be cured. As the cancer becomes more advanced, the cure rate declines, but it may still be treatable for long periods of time.
Most rectal cancers start as polyps, or growths. Over time, some, but not all, polyps change into cancers. Polyps that have a higher risk becoming cancer are known as adenomas.
Screening is extremely important, because finding polyps before they become cancerous reduces the risk of developing rectal cancer by at least 90 percent.
Finding ways to prevent polyps from forming is an important part of ongoing research at Dana-Farber Brigham Cancer Center.
Incidence
Together, rectal and colon cancers are the fourth most common type of cancers in the United States.
Rectal cancer is mainly a disease of developed countries with a Western culture.
It is most often diagnosed in people age 50 and older. However, it can affect those who are younger. Incidence appears to be increasing among younger people, though the reason for this is not known.
Rectal cancer affects men more than women.
There are about 40,000 new cases of rectal cancer each year in this country.
Risk Factors
Anything that increases your chance of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors does not mean that you will not get cancer. Risk factors for rectal cancer include:
Increasing age: Most people who develop rectal cancer are 50 or older.
A family history of cancer of the rectum or colon.
Certain hereditary conditions, such as familial adenomatous polyposis, and hereditary nonpolyposis colon cancer, called Lynch syndrome.
A history of inflammatory bowel disease (IBD), such as ulcerative colitis and Crohn's disease.
A personal history of cancer of the rectum, colon, ovary, endometrium, or breast.
A personal or family history of adenomas (polyps) in the rectum or colon. These growths can be pre-cancerous. Most adenomas will not turn into cancer. However, regular screening to remove them reduces the risk of developing rectal cancer.
Environmental and lifestyle-related factors, such as lack of exercise, obesity, smoking, and alcohol consumption.
Our team works on research with the Harvard T.H. Chan School of Public Health and has published many landmark papers on diet and lifestyle and risk of colon cancer.
A diet high in red and processed meat.
Low vitamin D levels.
Our team has published many studies on this; we are currently conducting several trials testing the role of vitamin D in the treatment of rectal cancer.
According to research conducted at Dana-Farber Brigham Cancer Center, 70 to 80 percent of rectal cancer cases may be prevented through exercise, weight control, limiting alcohol consumption, and taking aspirin and vitamin D. Learn more about the importance of exercise and good nutrition in cancer prevention and for cancer patients and survivors.
People with a family history of rectal cancer and/or other cancers in several close relatives across generations, especially if these cancers occur at a young age, may benefit from genetic counseling and testing. To learn more, visit our Center for Cancer Genetics and Prevention.
Symptoms and Signs
Potential symptoms and signs of rectal cancer include:
A change in bowel habits.
Blood (either bright red or very dark) in the stool.
Anemia (low red blood cell count).
Diarrhea, constipation, or feeling that the bowel does not empty all the way.
Stools that are narrower than usual.
Rectal pain.
Frequent gas pains, bloating, fullness, or cramps.
Weight loss for no known reason.
Feeling very tired.
It is important to know that these symptoms and signs can have many causes and may not be due to cancer. However, it is important that you discuss these symptoms or signs with your doctor.
Further, many people, particularly those with early stages of rectal cancer, may not have any symptoms or show any signs. This makes it difficult to detect without regular screening. Several screening methods make it possible to find some cancers before symptoms appear.
Screening and Prevention
Screening for rectal cancer helps prevent the disease and decrease the number of deaths from it. Some tests to find polyps can actually prevent the development of cancer because doctors can remove the growths before they become problems.
There are several ways to screen for rectal cancer. Each type of test has advantages and disadvantages, due to the risks, sensitivity, and accuracy of the test. You should talk to your doctor about when to begin screening for rectal cancer, what test to have, the benefits and drawbacks of each test, how often to undergo screening, and when to stop screening.
Options for screening include:
Colonoscopy: A procedure to look inside the rectum and entire colon for polyps, abnormal areas, or cancer. A colonoscope is inserted through the rectum into the colon. A colonoscope is a thin, tube-like instrument with a light and a lens for viewing. It will also have a tool to remove polyps or tissue samples, which are checked under a microscope for signs of cancer.
Digital rectal exam: An exam of the rectum. The doctor or nurse inserts a gloved finger into the rectum to feel for lumps or anything else that seems unusual.
DNA test: The stool is examined for small pieces of DNA that come from cells lining the colon and rectum. Abnormal DNA may be due to cancer.
Fecal occult blood testing: A test to check stool (solid waste) for blood that can be seen only with a microscope. Small samples of stool are placed on special cards and returned to the doctor or laboratory for testing.
Sigmoidoscopy: A procedure to look inside the rectum and sigmoid (lower) colon for polyps (small areas of bulging tissue), other abnormal areas, or cancer. A sigmoidoscope is inserted through the rectum into the sigmoid colon. A sigmoidoscope is a thin, tube-like instrument with a light and a lens for viewing. It also has a tool to remove polyps or tissue samples, which are checked under a microscope for signs of cancer.
Virtual colonoscopy: A procedure that uses a series of x-rays called computed tomography (CT) to create detailed images that may show polyps and anything else that seems unusual. This test is also called colonography or CT colonography.
Double-contrast barium enema: A series of x-rays of the lower gastrointestinal tract. A liquid that contains barium (a silver-white metallic compound) is inserted into the rectum. The barium coats the lower gastrointestinal tract and x-rays are taken. This procedure is also called a lower GI series. It is rarely used anymore.
Dana-Farber's Jeffrey Meyerhardt, MD, talks about symptoms, screening, and what you can do to prevent colon and rectal cancer.
Why Choose Us
Sapna Syngal, MD, MPH, is a gastroenterologist and Director of the Gastrointestinal Cancer Genetics and Prevention Program.
At the Colon and Rectal Cancer Center at Dana-Farber Brigham Cancer Center, our team of experts work together to provide compassionate, comprehensive, and highly coordinated care for patients with rectal cancer. Our specialists are world leaders in the field who create personalized treatment strategies based on extensive laboratory experience, as well as translational research.
We offer our patients with rectal cancer targeted therapies, clinical trials, advanced surgical procedures, and the full range of nutritional and other support services, from a top-ranked hospital and leading cancer research center.
We provide comprehensive services to patients with these cancers, including:
Personalized treatment plans: every patient treated as an individual with unique needs
The new Young-Onset Colorectal Cancer Center – one of the first centers in the country dedicated to treating colon and rectal cancer patients under age 50
Physician-scientists leading international studies of drugs that target the genetic drivers of rectal cancer, bringing you new and more effective treatments quickly
Multidisciplinary care delivered by specialists from Dana-Farber Cancer Institute and Brigham and Women’s Hospital